
Introduction of Interventional Radiology in Rwanda
Jeffrey Forris Beecham Chick, MD, MPH
Jeffrey Forris Beecham Chick, MD, MPH
Department of Radiology, Brigham and Women’s Hospital, Harvard Medical School, 75 Francis Street, Boston, Massachusetts 02115
Email: jchick@partners.org
{kind=link}

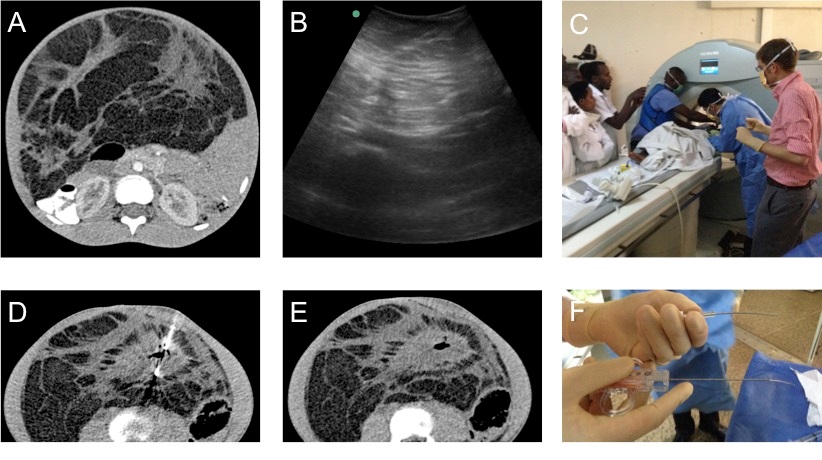
Today we performed the first ever computed tomography-guided biopsy in Rwanda. The patient was an 11-year-old female with large fat-containing abdominal mass which was concerning for a liposarcoma. Although the tumor was unlikely to be responsive to chemotherapy or surgical removal due to its advanced stage, the pediatric team requested the biopsy in an effort to have a definitive diagnosis prior to discharge home with palliation. Although the circumstances of this patient and case were certainly gloomy, there was a buzzing excitement throughout the radiology department as no one had performed or seen such a procedure in Rwanda. Our diagnostic radiology team arrived at 700AM. Anesthesia arrived at 830AM, although we requested the case start at 730AM, but a late start seems more of a cultural norm around here in Rwanda. Anesthesia provided procedural sedation with ketamine, which is different than we typically use in the United States, as our main population here in Rwanda is children unlike the adults we perform biopsies on at Brigham and Women’s Hospital. After the patient was anesthetized, my colleague, Nikunj Chauhan, and I donned our sterile attire, cleaned the patient’s skin, and placed the first “introducer” needle into the mass. A crowd of people, mainly doctors, nurses, and technologists watched as we worked, many taking cellular telephone photographs and videos. We took our first computed tomography scan and confirmed that the needle was indeed in the solid portion of the mass (which was necessary for confirming a diagnosis of liposarcoma). We then placed the biopsy device and took the first biopsy sample. There was intense anticipation as we waited to see what the sample looked like; it was white, indicating that we were likely in the tumor. The mass was much firmer than we anticipated, deforming the biopsy device, and pushing it out of the skin. Neither Nikunj nor I had experienced anything like this in the United States, but it raised the possibility that the tumor may be a desmoid, or fibrous tumor, rather than or originally proposed liposarcoma. Nevertheless, we continued on and took several additional samples of the mass. The large audience watched as we placed all of our samples in formalin. The procedure had gone well, without any complication, and we all felt as if we had done something beneficial for the patient as we placed her on the path to diagnosis. The disheartening part was that we’d have to wait 4-to-6 weeks to obtain the biopsy results
A: Pre-procedural computed tomography image demonstrating a predominately fat containing abdominal mass with several scattered islands of soft tissue concerning for liposarcoma.
B: Pre-procedural ultrasound image showing the ill defined infiltrating nature of the mass. Given an inability to adequately differentiate the soft tissue components under ultrasound, computed-tomography-guided biopsy was completed.
C: Intra-procedural photograph showing the setup and placement of the introducer needle in the first ever computed tomography-guided biopsy completed in Rwanda.
D: Intra-procedural computed tomography image demonstrating placement of the biopsy device within the soft tissue component.
E: Post-procedural computed tomography image demonstrating air within the soft tissue component confirming that the soft tissue component was indeed biopsied.
F: Photograph showing significant bending of the needles due to the hard nature of the mass raising the suspicion for a fibrous tumor such as a desmoid.
No comments:
Post a Comment